Various documentation is required in a healthcare facility. Nursing documentation is a fundamental requirement for recording a patient’s health status. Accurate nursing documentation ensures efficient patient care and communication.
Below are various documents to help record nursing data. Each worksheet is key, from monitoring vital signs to medication administration records. Sheets like wound care logs, neurological assessments, and sepsis screening tools enhance healthcare providers’ decision-making.
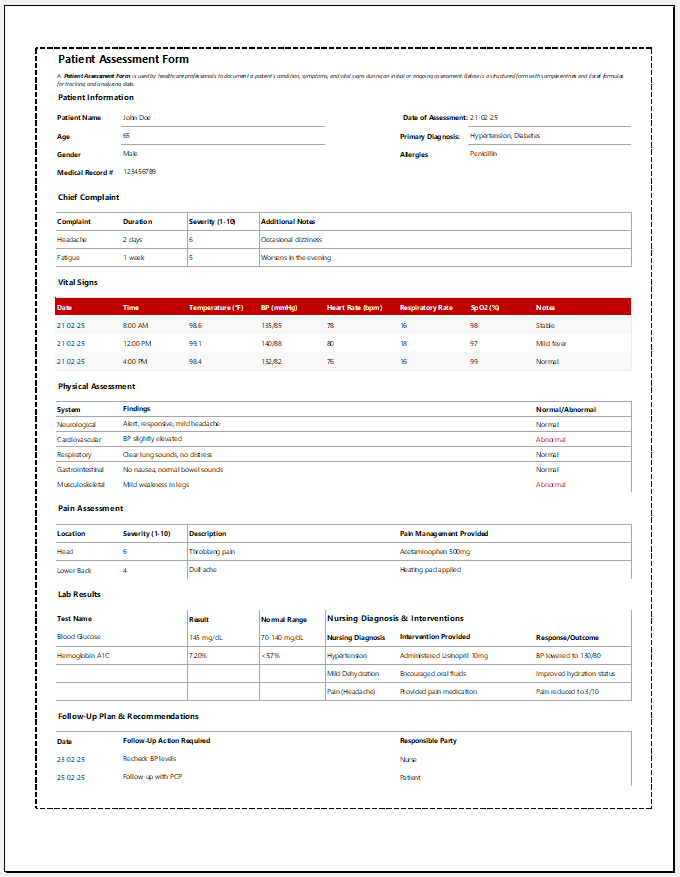
Patient Assessment Form
Healthcare professionals use a Patient Assessment Form to document a patient’s condition, symptoms, and vital signs during an initial or ongoing assessment.
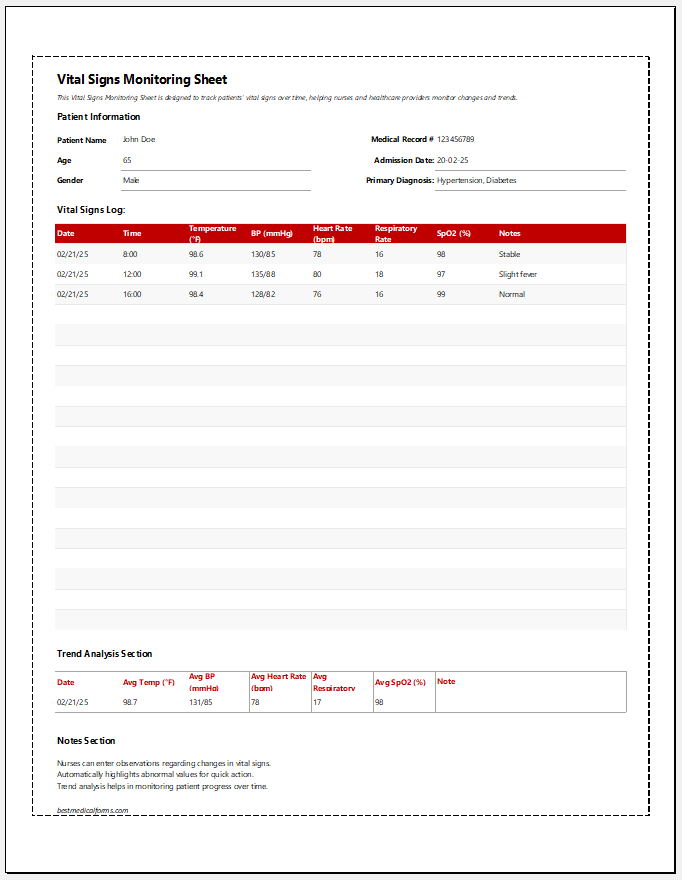
This Vital Signs Monitoring Sheet is designed to track patients’ vital signs over time, helping nurses and healthcare providers monitor changes and trends.
A Pain Assessment Log is used by nurses and healthcare providers to track a patient’s pain levels, characteristics, interventions, and responses over time.
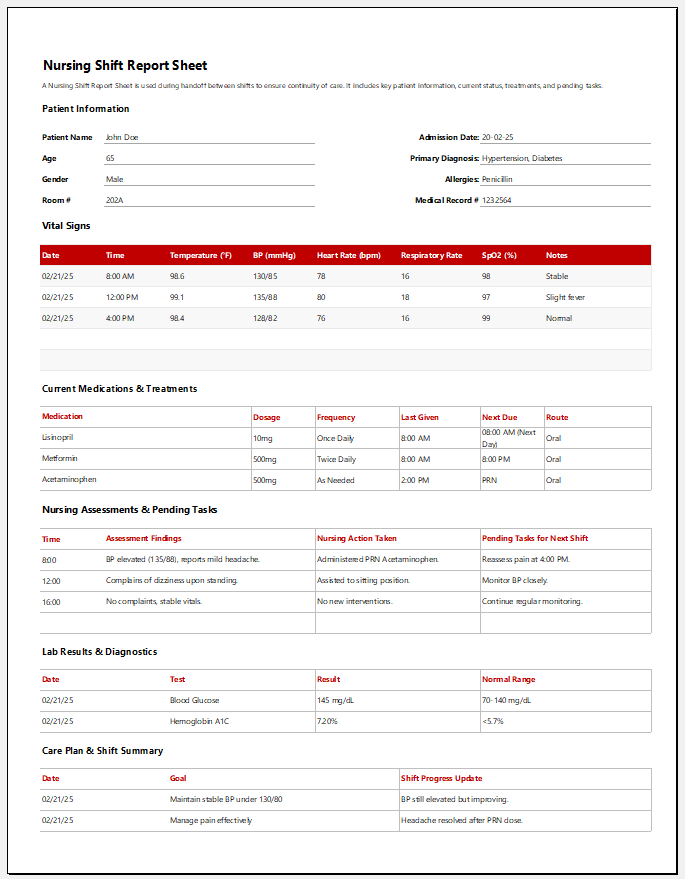
This Daily Nursing Notes Template provides a structured format for nurses to document patient progress, interventions, and responses throughout the shift.
A Fall Risk Assessment Sheet helps healthcare professionals evaluate a patient’s likelihood of falling, document risk factors, and implement preventive measures.
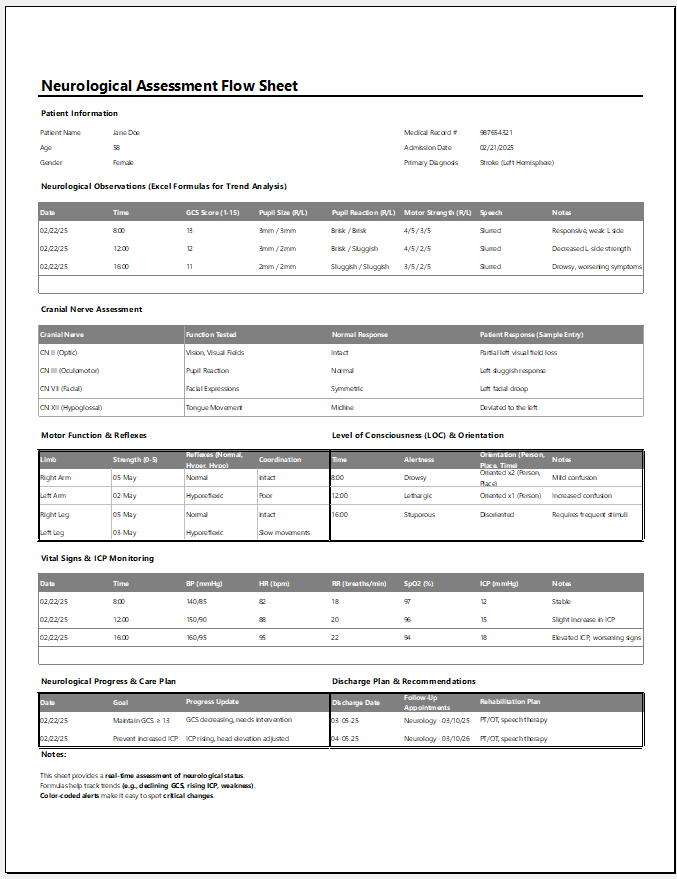
A Neurological Assessment Flow Sheet helps track a patient’s neurological status over time, allowing healthcare providers to detect changes and trends in mental status, motor function, pupil reaction, and vital signs.
The Labor and Delivery Nursing Chart tracks maternal and fetal health, labor progress, and postpartum recovery for accurate and efficient patient care.
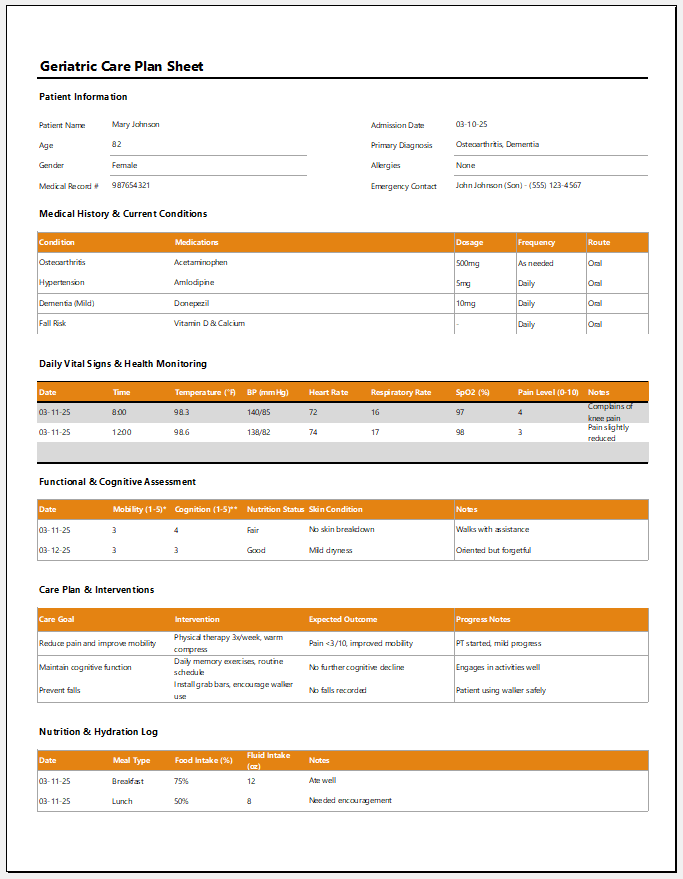
The Geriatric Care Plan Sheet is a document used to monitor elderly patients’ health, track interventions, and ensure comprehensive, personalized care.